Deep breath… here goes… We’re going to try and put together a concise ‘state-of-nation’ here on where the UK currently stands in terms of its fight against Covid.
The summer is over, public sentiment is hardening like the coming ice (hey, I live in the North, winters are harsh), and the information we’re being presented with is overwhelming, confusing and often either straight-up incorrect or deliberately obfuscated. In my humble and inexpert opinion, these factors leave us in the highest risk situation we have been in since the beginning of this crisis.
The Numbers
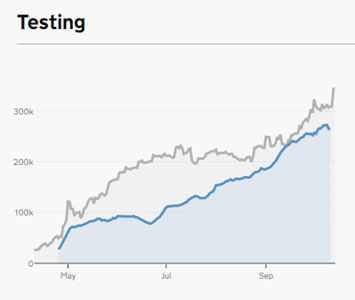
Let’s start with the raw, hard data first. One of the issues with our accounting and tracking of Covid-19 has been the evolution of testing; in March, April and May testing was largely limited to in-hospital targeted tests. This means our accounting of how many cases were in community circulation is virtually meaningless (some estimates put it at 10-20x the official figure), whilst we would expect the proportion of tests coming back positive to be extremely high at that time and dropping off as widespread testing was rolled out.
Despite an incredibly slow start, testing was ramped-up reasonably quickly, but it has been plagued by problems. For example, during the summer months testing was reliant on lab services being provided by Masters, PhD and postdoc candidates, who then went back to their normal roles as universities began to reopen, leaving the system with huge delays.
We’ve also counted these tests in highly questionable ways, with the government quoting the number of tests theoretically available on any one day as the number of tests taken for a number of months (or just straight-up counting them twice), this appears to have now been rectified.
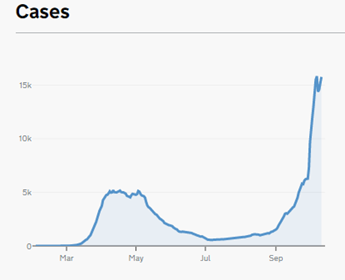
So on first glance the daily case numbers may show us to be in a far more serious situation than we were even at the peak in April, but this wouldn’t be a fair comparison. What should alarm us however is the case trajectory: we are now well established in the territory of the exponential. This means the R number is well above 1 and cases are spreading rapidly in community transmission.
To take this data out of isolation (‘scuse the pun) we need to consider hospital admissions and deaths. A common argument I am hearing is that the testing figures must be incorrect because they didn’t immediately precede a proportional jump in hospitalisations, but the relation between these figures is complex and influenced by a number of factors.
The first and most obvious is that people simply don’t get that ill straight away, there’s usually at least a few days between a positive test and hospitalisation, then it can be weeks before that same patient dies. Add in delays in reporting, and there is a serious lag between cases and deaths.
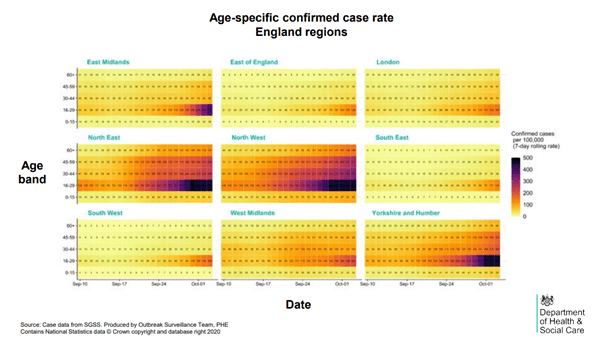
The second is the demographic factor: over summer younger people have been contracting the virus at a high rate. They have a habit of not getting particularly ill. As a critical mass of young people harbour a reservoir of Covid, the disease starts to slip through age demographics as shown in an age breakdown of cases. As the cases start to get to older people, we have begun to see the corresponding uptick in hospitalisation.
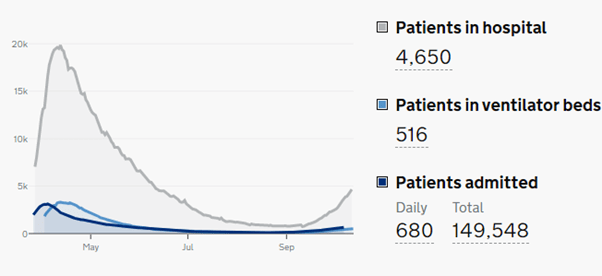
Looking at capacity, we appear to be a long way below the peak we previously experienced, but the national data belies regional variations; to take Liverpool as an example: as of 15th October 95% of ICU beds are occupied. That figure should be scaring the hell out of us.
To counter another point I hear regularly: that the death statistics are over-hyped due to the reporting method (depending on which statistic is being used at any one time, some cases are counted where there has been a death in the 28 days following a positive test), this is in theory a good point. Poor use of statistics erodes the credibility of these figures. But the point is moot when hospital beds are reaching capacity.
We should take a moment to celebrate the advances we have made in treatment of Covid-19; the use of tried and tested steroids such as dexamethasone have massively decreased ICU admission and increased ICU survival rates whilst we have much better understanding of how best to oxygenate patients. But those patients have still caught Covid-19 and still need a hospital bed and extensive aftercare.
What of the Nightingale hospitals then? Yes, these emergency makeshift wards provide a massive potential increase in bed capacity. No, they do not miraculously increase our available ICU trained doctors and nurses. As remarkable as their mobilisation was, nobody should be expecting first-class NHS care if we start to utilise them. Think more of a handful of harried, overworked, under-paid nurses, and teams of 18-year-old squaddies and cabin crew trying to keep you (or more likely your Gran) alive.
Risk, The Economy & Lockdowns
For those of us in our twenties the risks associated with socialising over summer have slipped into appearing vanishingly low. The chances of being hospitalised with Covid are slim and the date rate even lower. These collectively make any thought of further restrictions chafe like a jock-strap on the central line in summer.
Alas, once again it’s not that simple; even if we ignore that high levels of infection lead to transmission into higher-risk generations, evidence is emerging of the toll that the poorly understood ‘long Covid can take. At the moment there is little solid data to point to, but there are indications of four separate syndromes causing the affliction, some of which may turn out to me permanent. So to assume risk to younger, working-age demographics is low is still a foolish step to take without further study.
We do desperately need to keep as much of the economy open as we can, capital needs to continue flowing, and jobs need to be retained, lest we be left with a barren post-Covid economy after we’ve found a way to deal with this virus. The real problem with the economy of course is that nobody really understands how it works anymore; it’s all very much a “if we jump off the cliff but don’t look at the ground we won’t hit it” level of suspending disbelief. We do know though that keeping people working is good, both for GDP (don’t get me started on the endless growth delusion) which we need to keep throwing debt at hospitals and for everybody’s physical and mental wellbeing. But that cannot come at the price of allowing the disease to run rampant through the population – the collapse of the health system would be a disaster the likes of which recent generations haven’t seen.
There has been a huge amount of protest regarding the targeted shutdowns of the hospitality industry, the argument being that hospitality isn’t single-handedly spreading the disease. There are good arguments here, unfortunately hospitality has many factors working against it: large numbers of households gather in bars, pubs and restaurants, for extended periods of time. People eat and drink which necessitates removing masks, and they speak at elevated levels which encourages respiratory droplets to travel further. The final nail in the coffin has been the Autumnal weather, pushing patrons inside and shutting the windows – ventilation is proving to be absolutely key to reducing covid transmission.
This is where the abject failures of this government come in. With an effective and ‘world-beating’ test, track and trace system our control measures could have worked. But after many months and an astonishing £12bn spend, we still don’t have an effective system.
The Excel-gate scandal has shown that piss-poor implementation by incompetent outsourced teams has rendered us with a lack of intelligence. The long-awaited, much-lauded app still doesn’t integrate with some testing results systems, meaning positive cases can’t log themselves as such, so contacts won’t be alerted.
And so trust in covid-reducing restrictions, and the government in general, has faltered and we as a nation are becoming ever-less compliant. Half-arsed and incredibly complicated localised restrictions are feeding confusion and frustration. You need look no further for evidence than videos of Liverpool city centre on the eve of enhanced restrictions when it slipped into the ‘very-high’ category (whatever that means).
The people in that video aren’t malicious, they’re bereft of patience. They know that hospitality staff will go unsupported – most on minimum wage don’t stand a chance of paying their rent when they only receive two thirds of their wage. (And perhaps a sprinkling of cretins in there.)
Other regions are still in negotiations over what their local restrictions will be, the government equivocating and passing the buck to local authorities, whilst the days go on and transmission runs wild.
That’s not to say that in theory localised restrictions don’t make sense, a ‘one-size-fits-all’ approach would seem nonsensical, but the new tiered system in which the tiers are common (except when they’re not) and postcodes are changing tier by the hour is maddeningly complex. I’m genuinely not sure which tier I’m in, and I sure as hell don’t know the difference between them. I’m pretty sure I’m still allowed to go to Wales, but only before lunchtime?
I fear that all of this is shutting the stable door weeks after the corona horse has bolted. Slow reactions, incompetent government, and ignored scientific advisors are déjà vu from the mess of February and March. Johnson’s cabinet is trying once again to make everybody happy, which will surely lead to inevitably more strict restrictions to try and prevent the overwhelming of the health system. All this is the full knowledge that the full lockdown is taking a sledgehammer to the operating theatre because we let someone drive off with the scalpel. To full-on steal a tweet pointed out to me today: “There was no lockdown. Middle class people hid indoors while working class folks brought them stuff”.
My two-cents? We’ve fucked the duck on this. And I say we, because we’ve all played a part. We all had a sense of relaxation over summer that we could push at those restrictions, a view that was reinforced by our leaders doing exactly the same and failing totally to use that time to put measures in place that would keep our heads above water this winter.
So by all means, let’s hope for the best. Let’s try our hardest to make sense of these new restrictions (no mean feat), but let’s not be surprised if shit gets real in a few weeks.
I’ll end this diatribe with a cliché: stay safe.
